
The heart is the first internal organ system that needs to be fully functional during mammalian embryonic development. Therefore, both the early patterning events of the embryonic heart as well as growth and maturation of the various cardiac compartments during embryonic, fetal and postnatal life are imperative for survival of the organism.
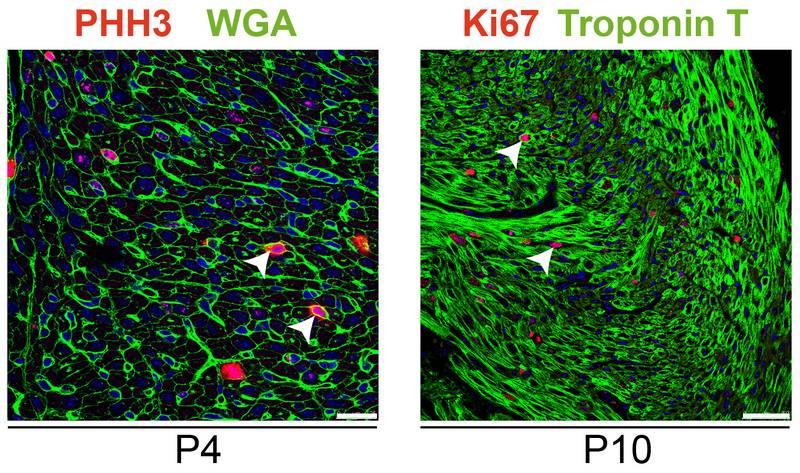
The basic growth patterns applied by the prenatal heart differ significantly from those utilized by the postnatal heart. In mammals, a unique feature of embryonic and fetal cardiomyocytes in contrast to adult cardiomyocytes is their ability to rapidly divide. This proliferative potential, however, ceases in late gestation and is lost shortly after birth such that postnatal cardiac growth is mainly achieved by cardiomyocyte hypertrophy. In rodents, the transition from proliferative to hypertrophic growth has been reported to occur within the first week of life whilst even earlier in larger mammals. Subsequently, terminal differentiation of adult cardiomyocytes results in irreversible cell cycle withdrawal precluding future cell divisions. This postnatal cardiomyocyte cell cycle arrest is widely believed to be a major cause for the inability of the adult heart to regenerate after injury.
In addition, the switch from proliferative to hypertrophic growth in the perinatal period is paralleled by significant changes in cardiac metabolism. During embryonic and fetal stages of mammalian heart development carbohydrates (i.e. glucose and lactate) are the primary energy source of cardiomyocytes. Therefore, the prenatal heart very much relies on glycolysis to meet the metabolic demands of the myocardium while glucose oxidation rates in mitochondria are low due to the low oxygen environment in utero. Immediately after birth a dramatic increase in fatty acid oxidation occurs in the heart which is paralleled by a decrease in glycolytic rates. Further maturation of the myocardium finally establishes oxidative phosphorylation in mitochondria fueled by carbon sources from fatty acid as well as glucose oxidation as the major energy source generating more than 95% of ATP within the heart. The switch from pre- to postnatal cardiac energy sources on the one hand and from proliferative to hypertrophic growth on the other hand is incompletely understood, but both processes are likely to be interdependent. Consequently, we are currently investigating the molecular and cellular changes occurring in the mouse heart in the immediate perinatal period. We are analysing gene and protein expression as well as signalling pathways involved in cell cycle regulation, growth and metabolism in late gestation foetuses compared to neonatal hearts. The expected findings will strengthen our general understanding of normal growth and maturation of the heart, but should also have implications for preterm birth, a condition which causes a premature exposure of the heart to the postnatal environment. The important questions in this regard are: How does the immature fetal heart cope with extrauterine conditions in terms of growth and metabolism and what are the long term consequences for the offspring later in life?
The final size of the adult heart is tightly controlled in relation to overall body size resulting in constant heart weight to body weight ratios among different individuals. Given the low cardiomyocyte turnover rate in the adult heart, postnatal growth relative to the size of the organism is almost exclusively achieved by an increase in cardiomyocyte size without a significant generation of new cells. An intriguing question in this regard is: How does the heart sense its own size and determine when to stop (or continue/resume) growth?
We are addressing the question utilizing the Hccs knockout mouse model described above (see project 1). Despite embryonic regeneration, hearts of neonatal cHccs+/- females are hypoplastic at birth, evident as a reduction in heart weight, thinning of left ventricular (LV) walls and a significantly reduced number of cardiomyocytes compared to littermate controls. The reduction in LV mass, however, normalizes until adulthood and this could be attributed to an increase in cardiomyocyte size (hypertrophy) in cHccs+/- females (while proliferation rates are unaltered indicating that cellnumber is not normalized). These data suggest the activationof compensatory cardiac growth mechanisms inthe postnatal heart after disturbed heart development allowing for normalization of cardiac organ size.Investigation of the underlying molecular mechanismsrevealed alterations of severalmetabolic regulators, such as mTOR (mechanistic target of rapamycin) and AMPK (AMP activated protein kinase), as wellas activation of pathways involved in protein homeostasis andamino acid metabolism in developmentally impaired hearts compared to controls. Using genetic and pharmacological tools we are currently trying to identify the functional relevance of the most promising candidates for both normal as well as compensatory cardiac growth and organ size control. These studies should increase our understanding regarding the consequences of impaired intrauterine development or preterm birth for the heart during postnatal life.